
Events / Education
International Cancer Imaging Society Meeting and 20th Annual Teaching Course
Tue 29 Sep 2020 Thu 01 Oct 2020 Society
Royal Society of Medicine, London, UKRelevant Documents
Main ProgrammeLearning objectives
To improve your knowledge of:
• Cancer diagnosis
• Cancer staging
• Response assessment
• Post-procedural assessment
• Emergency / side effects / complications of oncologic therapies
• Interventional radiology in oncologic patients
• Structured reporting
• Imaging protocols in cancer imaging
• Differential diagnosis of focal lesions
High quality educational lectures and hands-on workshops
• Refresh your knowledge of cancer imaging and learn about cutting edge developments
• Learn about state of the art multimodality cancer imaging using MRI, CT and PET
• Improve your knowledge of the mechanism of different drugs used in the treatment of cancer
• Bring your knowledge into practice in workstation based teaching in our hands-on workshops
• Focus on interventional radiology in oncology: from diagnosis to treatment
• Experience the role of cancer imaging in multidisciplinary interaction: treatment selection, early response prediction and treatment adaptation
• Learn how big data initiatives are changing the future of cancer imaging: radiogenomics, machine learning, AI
In addition:
• Presentations of cases you would like to read again
• Proffered papers (oral, poster and case-based presentations)

Venue: Royal Society of Medicine, 1 Wimpole Street, London, W1G 0AE
Tuesday 29th September to Thursday 1st October 2020
Keynote lectures
• Seeing is believing
• Cancer survivorship - imaging implications
• Harnessing the human genome
Plenary sessions – State of the Art Oncological Imaging
• Artificial intelligence
• Lymphoma
• Imaging techniques
• Radiation therapy
• Royal College of Radiologists session: Education and training
• Surgical and focal therapies
• Cancer genetics
• Interventional oncology
• Mimics of malignancy
Oncological Imaging - Practical Approach
• Diagnosis
• Imaging strategies in gynaecological malignancies
• Staging
• Response assessment
• Follow-up
Computer hands-on workshops
• PI-RADS v2.1
• Lung / Chest
• CT/MRI LI-RADS
• Characterising soft tissue masses - retroperitoneum to the extremities. A systematic approach.
• Colorectal MRI
• Whole-body MRI
Interactive workshop
• Focal renal lesions
Scientific paper sessions and poster exhibition
Prizes for the best oral presentations and best posters will be awarded at the course party on Wednesday evening.
HOW TO REGISTER
Online: Click for ONLINE REGISTRATION here to register.
Socials :
A complimentary Welcome Reception will take place after lectures on Tuesday 29th September at the Royal Society of Medicine.
The Course dinner will be held on Wednesday 30th September at the nearby Royal College of Physicians next to Regents Park from 19:30.
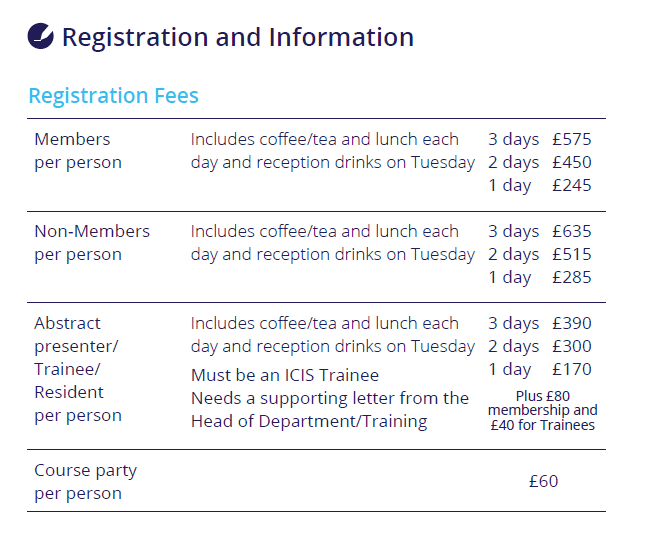
Delegates are invited to purchase a ticket for £60 per person You are welcome to purchase additional tickets for guests.
The closest underground stations to the Royal Society of Medicine are Oxford Circus (Bakerloo, Central and Victoria Lines) or Bond Street (Jubilee or Central Lines).
Arriving by air
The Royal Society of Medicine is within easy reach of all of London's major airports: Heathrow, Gatwick and Stansted (and to a lesser extent, Luton).
The Heathrow Express offers a fast service between Heathrow Airport and London's Paddington Station. From Paddington Station you can travel directly to Oxford Circus using the Bakerloo Line .
The Gatwick Express offers a fast service between Gatwick Airport and London's Victoria Station.
From Victoria Station you can travel directly to Oxford Circus using the Victoria Line
The Stansted Express offers a fast service between Stansted Airport and London's Liverpool Street Station.From here you can travel directly to Oxford Circus using the Central Line.
Arriving by train
Many main rail stations link directly to Oxford Circus, including Kings Cross, St Pancras, Euston Marylebone and Waterloo Stations.You can have a look at this tube map to plan your route.
Arriving by car
We do not advise people to travel in to the central London Area by car as parking can be difficult. However further information is available on the following sites.
Parking information : http://en.parkopedia.co.uk
Paying the Congestion Zone: http://www.tfl.gov.uk/roadusers/congestioncharging/
Travelling around London
For more information public transport in London: http://www.tfl.gov.uk/
Royal College of Radiologists – delegates will receive 18 credits in total for the three-day course. Tuesday 6.5 credits, Wednesday 6.5 credits, Thursday 5 credits.
Accreditation for CME points has been applied for from the European Accreditation Council for Continuing Medical Education (EACCME).
American delegates can have their EACCME European CME Credits converted to AMA PRA Category 1 Credit™ by applying to the AMA.
Download the 1 page from here:- https://www.ama-assn.org/sites/default/files/media-browser/public/cme/eaccme-application.pdf
Send the completed form to the AMA together with the EACCME certificate* and the non-refundable processing fee (AMA members $30 and non AMA members $75). AMA certificates will be emailed within 3 business weeks.
* The EACCME certificate will be automatically emailed to you once you have completed the ICIS course daily electronic surveys.
Please visit this link for further information https://www.ama-assn.org/education/uemseaccme-cme-credit-recognition
» Guidelines » Examples » Download Abstract Guidelines
General Rules
Abstracts that do not adhere to the following important points will be rejected:
> The title should not exceed 15 words. The title should be in bold, sentence case with no full stop at the end and no underlining.
> The abstract should not exceed 250 words.
> Please use authors’ initials and surnames only. No full stop at the end. Underline the name of the corresponding author. A comma should separate author names. Where authors are from a number of different institutions, the appropriate institution number from the affiliation list should be given as a superscript number immediately after each author's name, e.g.: John Smith1, Susan Jones1, Bill Fisher2. An asterisk * should be used to link the corresponding author with their email address
> Affiliations should include institute, town and country. Where there are multiple affiliations, each should be listed as a separate paragraph. Each institute should appear in the order used against the author names (see above paragraph) and show the appropriate superscript number, e.g.:
1 University, Town, State, USA
2 University, Town, UK
2 Company, Town, Country
> Qualifications should be omitted.
> Do not include references, tables or figures.
> Please do not use block capitals.
Main text
> In structured abstracts, paragraph headings should be typed in bold with no colon at the end. Do not use the heading ‘Abstract’. Each heading should be in a separate paragraph.
Aim
Followed by regular text, on a new line and in the same format as shown above for main text.
Materials & Methods
Results
Conclusions
Consent to publish If the abstract contains details relating to individual participants (for example a case report), written informed consent for the publication of these details must be obtained from the participants and a statement to this effect should appear at the end of the abstract. Our guidelines for consent statements can be found here: http://www.biomedcentral.com/about/editorialpolicies#Ethics. If the patient is deceased consent for publication should be obtained from the next of kin and if the patient is under 16 consent should be obtained from the parent or guardian.
Please find examples at the bottom of the page.
You may choose among four different abstract types:
> Oral Scientific Presentation
> Oral Case Based Presentation
> Poster Scientific Presentation
> Poster Educational Presentation
Oral Scientific Presentation
The abstract should be separated into “Aim”, “Methods”, “Results” and “Conclusion”. The abstract limit is 250 words. Abstracts should not include promissory notes such as “We will provide additional data during our presentation.” Authors of accepted oral presentations will be invited for a presentation within the Scientific Paper Sessions. Presentation time will be 8 minutes with 2 minutes for Q&A (depending on the final program).
Oral Case Based Presentation
The abstract should have an image and three teaching points. The abstract limit is 250 words. Abstracts should not include promissory notes such as “We will provide additional data during our presentation.” Authors of accepted oral case based presentations will be invited for a presentation within the Scientific Paper Sessions. Presentation time will be 8 minutes with 2 minutes for Q&A (depending on the final program).
Poster Scientific Presentation
The abstract should be separated into “Aim”, “Methods”, “Results” and “Conclusion”. The abstract limit is 250 words.
Poster Educational Presentation
The abstract should be separated into “Learning Objectives”, “Content Organisation”, and “Conclusion”. The abstract limit is 250 words.
Proceedings of the 20th International Cancer Imaging Society Annual Teaching Course
Abstracts selected for presentation will be published in the Proceedings of the 20th International Cancer Imaging Society Annual Teaching Course, given to all delegates and faculty. A downloadable version of your submission will be made available to our membership on the members only area of our website, and be available on the Cancer Imaging open access website. Authors of selected abstracts will be notified after Friday 3 July 2020.
It will be obligatory for all scientific presenters to be members of ICIS at the time of presentation. The annual membership fee of £80 will be added to the scientific presenters’ fee at registration if current membership is not in place. Please note that we have a discounted trainee membership at £40 for those who send a letter from their head of department, confirming their status as Head of Department. Membership will run for one year from date of registration; all standard member benefits will apply.
Financial help will be available for junior proffered presenters. This will be decided on application and on a case-by-case basis.
Applicants for financial aid please email [email protected] for further information.
Queries may be addressed to the ICIS Secretariat
Tel: +44 (0) 7956 814964 or Email: [email protected]
Submission deadline: Monday 1st June 2020
EXAMPLE – ORAL CASE BASED PRESENTATION
Diagnosis: Advanced Cervix Cancer
Sala E.
Memorial Sloan Kettering Cancer Center, New York, USA
Images:

Teaching/Discussion points:
> Discuss the role of MRI in treatment slection and planning of patients with cervical cancer
> Describe MRI Features of parametrial and pelvic sidewall invasion
> Highlight potential pitfalls
EXAMPLE - POSTER EDUCATIONAL
Chemotherapy induced cardiomyopathy: an overview, imaging features, and future prospective
Firstname A Lastname1*, Firstname B Lastname2, Firstname C Lastname3
1University, Town, State, USA
2University, Town, UK
3Company, Town, Canada
*Email address of corresponding author if being included
Learning objectives:
To review the spectrum of imaging findings of chemotherapy- induced cardiomyopathy in correlation with most common cytotoxic drugs and regimens.
Content organisation:
Cardio toxic effect of chemotherapy is a well-recognized problem in cancer patients. Cardio toxicity depends on multiple predisposing factors, specific components of the chemotherapy regimen, length of treatment, and dosage.
We will present the spectrum of most common cardiotoxic chemotherapy agents and their combinations, specific effects on the myocardium, and imaging features of cardiomyopathies induced by chemotherapy.
We will review pathophysiology of chemotherapy induced cardiomyopathy including:
- Dose dependent cardiomyopathy
- Predisposing conditions –diabetes, presence of coronary artery disease, age.
- Potential reversibility
We will discuss imaging characteristics of chemotherapy induced cardiomyopathy
- Imaging modalities ( Echocardiography, Cardiac MR, and MUGA)
- Importance of monitoring cardiac function during and after treatment
- Distribution of late Gadolinium enhancement (LGE)
- Emerging technologies for early diagnosis of cardiomyopathy in cancer patients
Conclusions:
Chemotherapy induced cardiomyopathy is a common problem among cancer patients, increasing long term morbidity and mortality and often leading to disability. Patients receiving chemotherapy treatment, particularly cardio toxic agents, should be routinely assessed for cardiac function to diagnose cardiomyopathy during the early phase of treatment and to prevent development of irreversible heart failure.
EXAMPLE POSTER SCIENTIFIC
The value of 68Ga-PSMA enhanced MR-PET in patients with biochemical recurrent prostate cancer
Firstname A Lastname1*, Firstname B Lastname2, Firstname C Lastname3
1University, Town, State, USA
2University, Town, UK
3Company, Town, Canada
*Email address of corresponding author if being included
Aim: In patients with prostate Cancer increased levels of PSMA can be measured. Recently a new tracer, 68Ga-PSMA, was developed as a specific marker for hybrid imaging (PET/CT, MR-PET). In this study we evaluated the accuracy of 68Ga-PSMA in patients with rising PSA after radical prosatectomy, so called „biochemical recurrent prostate cancer“ (BRPC).
Materials and Methods: A total of 322 patients with BRPC underwent a MR-PET examination (Siemens Biograph mMR) after injection of about 150 mBq 68Ga-PSMA. Images were evaluated in cosensus by one experienced nuclear medicine physician and one radiologist. Pelvine lymphnode dissection was performed in most of the patients according to a predefined template with 8 fields. Lymphnode involvement was evaluated according to a 5 point scale with a patient- and a field-based analysis. These findings were startified according to PSA-values.
Results: Four patients were excluded from the study for different reasons. Sensitivity for detction of recurrence was 95.7 % for PSA-values ≥ 2ng/ml, 81.4 % for PSA-values of 1-2 ng/ml, 76% for PSA-values 0.5-1 ng/ml, and 51% for PSA values ≤ 0.5 ng/ml. In comparison to the MR-images alone MR-PET was of superior diagnostic value.
Conclusions: MR-PET using 68Ga-PSMA is a sensitive and highly accurate technique for the diagnosis of biochemical reccurence of prostate cancer after radical prostatectomy. It yields high diagnostic performance at relatively low PCA-values.
|
Don’t take our word for it. Read what our delegates said about our 2019 annual teaching course: • I found all the lectures useful and informative with a lot of information that can be integrated in daily practice . The venue, lecturers and support staff were exceptional and the gala evening was absolutely superb!!! Thank you for your hard work and making this possible. . • In our practice nobody wants to miss ICIS. Because the well-prepared lectures on multi parametric hybrid imaging help us understand tumour biology. • Extremely interesting conferences and workshops, great faculty. Well organised in every aspect. • One of my favourite meetings. Great locations, not too big, some outstanding speakers and all the latest in cancer imaging in one place. There's something for everyone who reports cancer scans here; from general to sub-specialists. A friendly faculty always helps too. |
|
Meeting Sponsors
|




")